Sridevi e-log
This is an online E-log book to discuss our patient’s de-identified health data shared after taking his/her/guardian signed informed consent.
Here we discuss our individual patient’s problems through series of inputs from available global online community of experts with an aim to solve these patient’s clinical problems with collective current best evidence based inputs.
This e-log also reflects my patient-centered online learning protfolio and your valuable inputs on comment box is welcomed.Hey
Here is the case i have seen:
A 60yr old male came to the hospital on with the chief complain of head ache and neck pain since 10 days,tingling sensation of both foot since 1 day,slippage of footwear and burning micturation since 1day
History of present illness:
Pt was apparently asymptotic 10 days back ,then developed fever for one day associated with body pains for which he went to RMP,took medication (unknown) in the afternoon.There is an episode of giddiness in evening and sustained trauma while walking due to slippage.
No h/o loc,ent bleed,blurring of vision,vomiting ,seizures following trauma but complaining of headache since then.
No h/o weakness of upper and lower limbs,no h/o difficulty in getting up from squatting position,combing hair,buttoning and unbuttoning,wearing chappal
Complaining of slippage of footware while walking since morning
Assosciated with cotton wool sensation and tingling sensation in bilateral foot
No h/o vomiting,loose stools,pain abdomen,increase or decrease in urine output ,cough,sob,chest pain,palpitations
Past history :
K/c/o hypertension since 5 yrs on T.telma -AM(40/5) OD
Diabetes since 5 years on T.glimi-MI OD
Not a k/c/o asthma , jaundice,epilepsy
Personal history :
Alcoholic since 40 yrs,4-5times per month,90ml
Drug history:
T. Telma-AM since 5 yrs
T. glimi-MI since 5 yrs
General Examination:
Pt is conscious,coherent,cooperative
moderately built ,moderately nourished
Vitals - Temp-Afebrile
BP-120/70mmhg
PR-82bpm
RR-18cpm
Grbs-245mg/dl
CNS examination:
Higher mental functions: pt is conscious ,speech is normal
Motor system:
Bulk: Rt Lt
UL- N N
LL- N. N
Tone:
UL- N. N
LL- N N
Power:
UL- 5/5 5/5
LL- 5/5 5/5
Reflexes:
Triceps reflex- 2+
Biceps reflex-1+
Supinator reflex-2+
Knee reflex-absent on both sides
Ankle reflex-absent on both sides
Plantar reflex-extended
Sensory system:intact
Cranial nerves:intact
No cerebellar signs
No signs of meningeal irritation


Respiratory system:
Shape of chest is normal, trachea is central in position,b/l air entry is present,no added sounds
CVS:
S1 S2 heard , no murmurs ,jvp is normal,no parasternal heave ,palapble trills
Per abdomen:
Shape of abdomen-distended
Waist circumference-116cms
No local rise of temperature and no tenderness,no palpable mass ,no visible peristalsis,hernial orifices are free, no organomegaly,bowel sounds heard





Hb-11.8g/dl
Rbs-84mg/dl
Cue- albumin +
sugar ++
pus cells=4-5
epithelial cells=2-3
Serum creatinine -0.9
Serum electrolytes- Na-137mEq/l
K-4.3mEq/l
Cl-95mEq/l








Diagnosis:
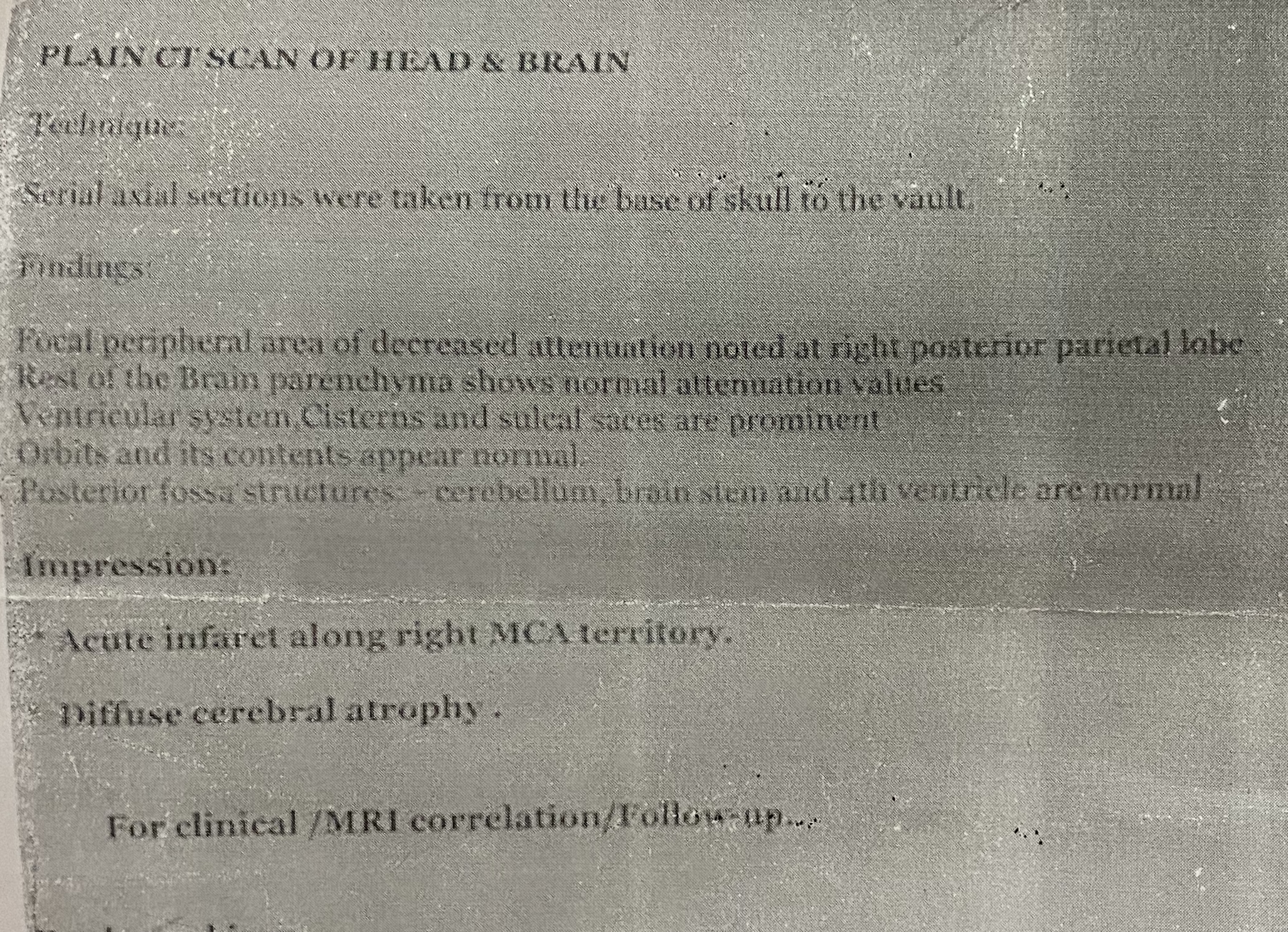
Chronic RMCA infarct
Transient ischemic attack
Uncontrolled diabetes mellitus
K/c/o HTN
Treatment:
Tab.ecospirin -AV 75/20mg PO OD
Tab.clopidogrel 75mg OD
Tab.pregabalin 75mg OD H/S
Tab.telma 40mg OD
Tab.pcm 650mg PO OD
Inj.human actrapid insulin s/c
Acc to sliding scale
8am—2pm—8pm
Grbs charting 6th hrly
Moniter vitals
I/o charting
Discussion:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4146153/
The American Heart Association has revised the proposed definition of TIA to a tissue-based term without time limit, previously 1 hour. The recent definition of a TIA includes “any neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction” (Easton et al., 2009), of typical symptom duration of less than 1 to 2 hours. According to this definition, a prolonged TIA might occur. Diagnostic correctness depends on the extent of the evaluation.

Comments
Post a Comment